Chapter 20 Anesthesia, Disorders of Consciousness, and Altered States
20.1 Chapter Overview
Theories of consciousness must explain not only ordinary waking experience, but also the many ways consciousness can fade, fragment, transform, or become disconnected from outward behaviour. Sleep, dreaming, anesthesia, coma, unresponsive wakefulness syndrome, minimally conscious state, locked-in syndrome, seizures, meditation, psychedelic states, and dissociation all reveal different dimensions of conscious life [@laureys2005; @owen2006; @seth2021].
Altered and impaired states are important because they show that consciousness is not a single all-or-nothing phenomenon. Wakefulness, awareness, responsiveness, reportability, memory, selfhood, sensory integration, and bodily presence can dissociate from one another. A person may be awake but minimally aware. A dreamer may be conscious while disconnected from the external world. A locked-in patient may be fully conscious but unable to move or speak. An anesthetized patient may show residual sensory processing without reportable awareness.
These dissociations make altered states some of the strongest empirical tests for theories of consciousness. A theory that explains only normal waking experience is incomplete. A successful theory must also explain how consciousness disappears under anesthesia, how it persists in dreams, how it may remain covert in some non-responsive patients, and how selfhood changes in meditation, psychedelic states, and dissociation.
This chapter examines altered and impaired states of consciousness as comparative windows into the structure of conscious experience. Particular attention is given to anesthesia, disorders of consciousness, dreaming, psychedelic states, meditation, dissociation, and the predictions made by major theories of consciousness.
20.2 Learning Objectives
After reading this chapter, the reader should be able to:
- Explain why altered states are important for consciousness research.
- Distinguish levels of consciousness from contents of consciousness.
- Describe major disorders of consciousness.
- Explain how anesthesia alters conscious processing.
- Compare dreaming and waking consciousness.
- Describe psychedelic and meditative alterations of perception, selfhood, and awareness.
- Analyze how different theories interpret altered states.
- Evaluate methodological and ethical challenges in altered-state research.
- Explain how altered states relate to the hard problem of consciousness.
20.3 Core Idea in One Picture
Figure @ref(fig:fig-altered) summarizes the major conceptual structure of altered and impaired states of consciousness.
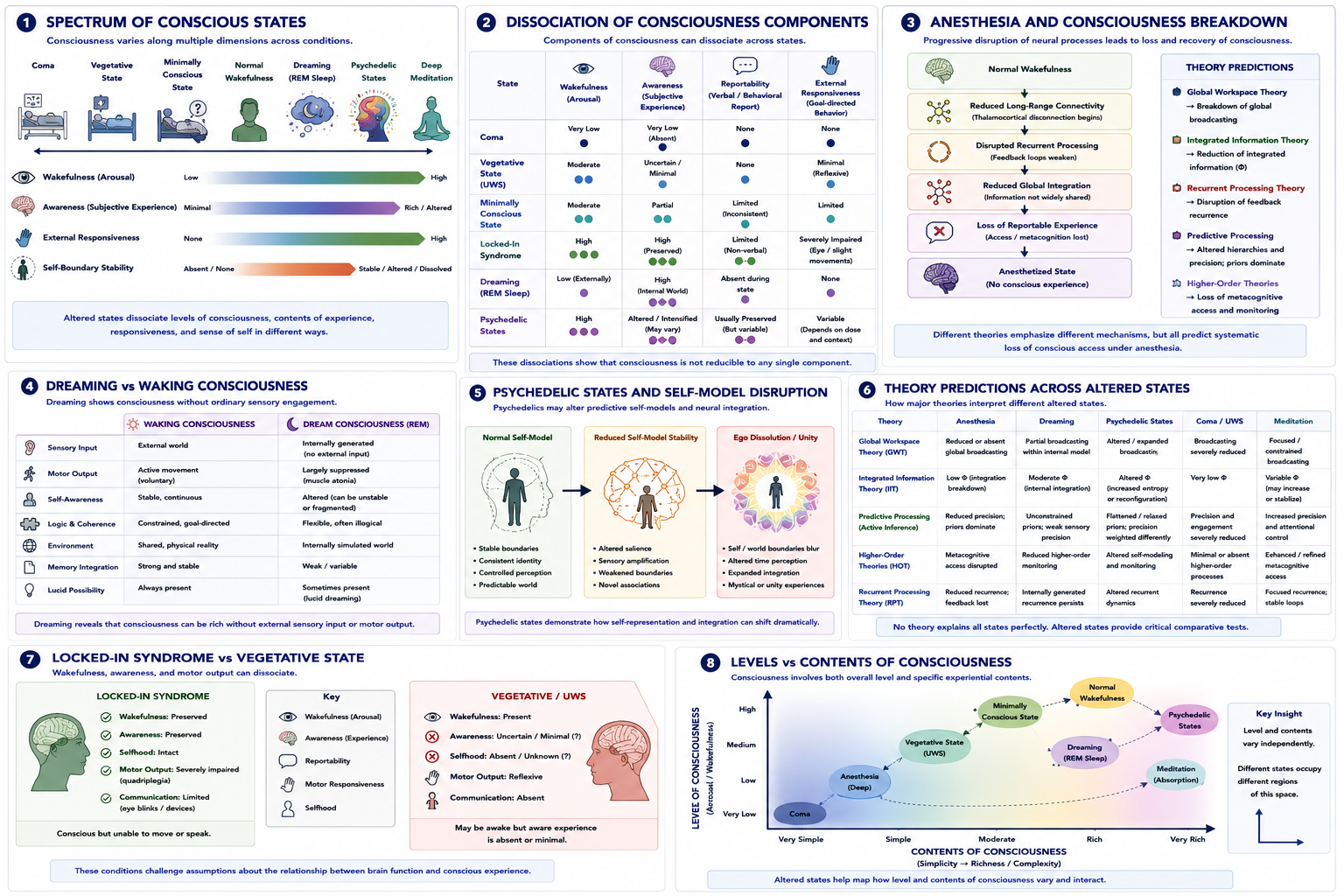
Figure 20.1: Anesthesia, disorders of consciousness, and altered states. Panel 1 illustrates the spectrum of conscious states. Panel 2 shows dissociation of consciousness components across conditions. Panel 3 explains anesthesia-related breakdown of consciousness. Panel 4 compares dreaming and waking consciousness. Panel 5 illustrates psychedelic disruption of self-modeling. Panel 6 compares theoretical predictions across altered states. Panel 7 contrasts locked-in syndrome with vegetative state. Panel 8 distinguishes levels and contents of consciousness.
As Figure @ref(fig:fig-altered) illustrates, altered states reveal that consciousness is multidimensional. Wakefulness, awareness, responsiveness, selfhood, memory, sensory integration, and reportability do not always rise and fall together. This makes altered states essential for understanding what consciousness is and how it depends on brain, body, cognition, and environment.
20.4 Why Altered States Matter
Altered states matter because they separate processes that usually appear unified in ordinary waking life. In everyday experience, wakefulness, perception, attention, memory, selfhood, and action often seem to belong together. Altered states show that these components can come apart.
For example, a person in a dream may have vivid experience while being largely disconnected from the external world. A patient in locked-in syndrome may be aware but unable to produce normal behavioural responses. A patient in an unresponsive wakefulness state may show wakefulness without clear signs of awareness. A person under anesthesia may lose reportable consciousness while some sensory processing continues [@laureys2005; @owen2006].
These cases help researchers distinguish the neural and cognitive processes associated with arousal, awareness, communication, selfhood, and conscious content. They also challenge simple definitions of consciousness based only on behaviour or verbal report.
Altered states therefore function as natural and clinical experiments on consciousness. They reveal what happens when different dimensions of consciousness are selectively weakened, preserved, or transformed.
20.5 Levels and Contents of Consciousness
A central distinction in clinical consciousness research is the distinction between levels of consciousness and contents of consciousness.
Level of consciousness refers to the overall degree of arousal or wakefulness. A coma involves very low arousal. General anesthesia reduces consciousness in a controlled medical context. Ordinary wakefulness involves a high level of arousal.
Contents of consciousness refer to what is experienced. These include perceptions, thoughts, emotions, bodily sensations, dreams, memories, images, and self-awareness.
This distinction is important because level and content can dissociate. A person may have high wakefulness but altered contents, as in psychedelic states or certain meditative states. A person may have reduced wakefulness but internally generated contents, as in dreaming. A patient may show wakefulness without clear evidence of meaningful conscious content, as in unresponsive wakefulness syndrome.
The distinction can be summarized as:
level = how awake or aroused the system is
content = what is experiencedA complete theory of consciousness must explain both dimensions.
20.6 The Spectrum of Conscious States
Conscious states exist along a complex spectrum rather than a simple on-off switch. At one end are states such as coma, where wakefulness and responsiveness are absent. Other clinical states include unresponsive wakefulness syndrome, minimally conscious state, and locked-in syndrome. Ordinary waking consciousness occupies only one region of this broader landscape.
Dreaming, meditation, psychedelic states, seizures, dissociation, and other altered states show that consciousness can change in content, structure, selfhood, emotional tone, sensory vividness, and relation to the external world.
This spectrum can be represented roughly as:
coma → unresponsive wakefulness → minimally conscious state → wakefulness → dreaming → psychedelic states → contemplative altered statesThis ordering is only schematic. Different states vary along different dimensions. For example, dreaming may involve rich conscious content but low external responsiveness. Locked-in syndrome may involve preserved awareness but severely reduced motor output. Psychedelic states may involve high wakefulness with altered self-boundaries and perception.
The important point is that consciousness is multidimensional, not binary.
20.7 Anesthesia
Anesthesia is one of the most powerful tools for studying consciousness because it allows controlled reduction and recovery of conscious awareness. Under general anesthesia, patients lose ordinary reportable experience, responsiveness, and memory for the surgical period. This makes anesthesia a valuable model for investigating how consciousness depends on brain integration and communication [@alkire2008; @sanders2012].
Anesthesia is not simply sleep. It actively alters neural communication, cortical integration, thalamo-cortical dynamics, recurrent processing, and large-scale brain coordination. As anesthetic depth increases, long-range connectivity often weakens, recurrent interactions become disrupted, and global information sharing declines.
Different theories interpret anesthesia in different ways. Global Workspace Theory predicts a breakdown of global broadcasting and large-scale cognitive access [@baars1988; @dehaene2011]. Integrated Information Theory predicts a reduction in integrated causal structure [@tononi2004; @oizumi2014]. Recurrent Processing Theory emphasizes disruption of feedback and recurrent signaling [@lamme2006]. Predictive Processing emphasizes altered hierarchical inference and precision weighting [@friston2010; @clark2013]. Higher-Order theories emphasize disruption of metacognitive access and self-monitoring [@rosenthal2005; @lau2011].
Anesthesia therefore provides an important comparative test. A theory of consciousness should explain why anesthetic agents can abolish reportable experience while leaving some lower-level sensory and physiological processing intact.
20.8 Disorders of Consciousness
Disorders of consciousness are among the most challenging conditions in neuroscience and medicine. They reveal that wakefulness, awareness, responsiveness, and communication can dissociate dramatically.
Coma involves absence of wakefulness and lack of purposeful responsiveness. Patients in coma do not show normal sleep-wake cycles or clear evidence of awareness.
Unresponsive wakefulness syndrome, historically called vegetative state, involves wakefulness without clear behavioural evidence of awareness. Patients may open their eyes, show sleep-wake cycles, and display reflexive behaviours, but they do not show reliable signs of conscious command-following [@laureys2005].
Minimally conscious state involves inconsistent but reproducible evidence of awareness. Patients may show limited command-following, purposeful behaviour, emotional responses, or attempts to communicate.
Locked-in syndrome is different. Patients with locked-in syndrome may be fully conscious and cognitively intact, but unable to move or speak because of severe motor impairment. This condition demonstrates that absence of normal behavioural response does not necessarily imply absence of consciousness.
These disorders raise major diagnostic, ethical, and theoretical questions. They show why consciousness cannot be assessed by behaviour alone.
20.9 Covert Consciousness
Modern neuroimaging and electrophysiology have revealed evidence for covert consciousness in some patients who appear behaviourally unresponsive. In some cases, patients unable to communicate outwardly have shown brain activity patterns consistent with command-following.
A famous example involved asking patients to imagine playing tennis or navigating through their home while undergoing brain imaging. Some patients produced activity patterns similar to healthy conscious participants, suggesting preserved awareness despite lack of behavioural response [@owen2006; @monti2010].
These findings have profound implications. Clinically, they affect diagnosis, prognosis, communication, and care. Ethically, they raise questions about suffering, autonomy, consent, and end-of-life decisions. Theoretically, they challenge theories that rely too strongly on external report or overt behaviour.
Covert consciousness also shows why consciousness science must combine behavioural observation with neural measures, careful clinical assessment, and ethical caution.
20.10 Dreaming
Dreaming demonstrates that consciousness can occur without ordinary engagement with the external world. During dreams, people experience internally generated environments, emotions, narratives, images, and sometimes a sense of self, even while external responsiveness is greatly reduced [@hobson2000; @revonsuo2000].
Dreaming challenges theories that identify consciousness too closely with external behaviour or sensory input. Dreamers may be conscious, but their conscious world is largely generated internally.
Dreaming also raises questions about selfhood and rationality. Dream experience often includes altered logic, unstable identity, emotional intensity, and reduced reflective awareness. Yet dreams can still be vivid, meaningful, and subjectively real while they occur.
The comparison between waking and dreaming suggests that consciousness depends not only on external sensory input, but also on the brain’s ability to generate coherent experiential worlds.
20.11 Lucid Dreaming
Lucid dreaming occurs when the dreamer becomes aware that they are dreaming. This state is especially important because it introduces reflective awareness into the dream state.
In ordinary dreams, the dreamer usually accepts the dream world as real. In lucid dreams, metacognition partially returns. The person may recognize the dream as a dream and sometimes exert limited voluntary control.
Lucid dreaming is relevant to Higher-Order theories because it shows that metacognitive awareness can vary within conscious states. It is also relevant to Global Workspace Theory because lucid dreaming may involve increased cognitive access and self-reflection compared with ordinary dreaming.
Lucid dreaming therefore demonstrates that consciousness is not only about whether experience is present. It is also about how much reflective awareness, control, memory, and self-monitoring are present.
20.12 Psychedelic States
Psychedelic states produce major alterations in perception, emotion, selfhood, meaning, sensory integration, and temporal experience. They are scientifically important because they can strongly alter conscious content while wakefulness is preserved.
Commonly studied changes include intensified sensory experience, altered emotional salience, changes in bodily self-awareness, increased associative thinking, altered time perception, and weakening of ordinary self-boundaries. Some individuals report ego dissolution, meaning a reduced sense of separation between self and world [@carhartHarris2014; @carhartHarris2019].
Predictive Processing theories often interpret psychedelic states in terms of altered precision weighting and weakened high-level priors. On this view, ordinary perception and selfhood are stabilized by high-level expectations. Psychedelics may relax these expectations, allowing perception, emotion, and self-modeling to become more flexible or unstable [@carhartHarris2019; @friston2010].
Psychedelic research is important for consciousness science because it alters core features of subjective experience: selfhood, salience, sensory structure, emotion, and meaning. It should be discussed scientifically and carefully, without treating these states as simple enhancement or as evidence for any single metaphysical theory.
20.13 Meditation and Contemplative States
Meditative and contemplative practices can alter attention, self-awareness, emotional regulation, bodily awareness, and the sense of self. Some traditions describe states involving reduced self-referential thought, open monitoring, nondual awareness, altered time experience, and increased meta-awareness [@lutz2008].
Meditation is important for consciousness research because it shows that conscious experience can be trained and transformed. Attention can become more stable. Emotional reactivity can change. Bodily sensations may become more vivid. The sense of self may become less rigid or less narrative-based.
These states are relevant to multiple theories. Higher-Order theories can examine changes in metacognition and self-monitoring. Predictive Processing can examine changes in self-modeling and precision weighting. Embodied theories can examine bodily awareness and interoception. Global Workspace Theory can examine changes in attention and access.
Meditative states also intersect with consciousness-first frameworks, including T-Consciousness, when they are interpreted as revealing deeper or more fundamental dimensions of awareness. However, such interpretations should be presented carefully. From a scientific perspective, meditation provides data about altered attention and self-experience. Metaphysical interpretations require additional philosophical argument [@taheri2020; @taheri2023].
20.14 Seizures and Dissociative States
Certain seizure disorders can produce dramatic alterations in perception, memory, emotion, bodily ownership, and temporal awareness. Temporal lobe seizures, for example, may involve déjà vu, depersonalization, intense emotion, altered reality sense, or unusual self-experience [@northoff2011].
Dissociative states can also disrupt selfhood, memory integration, agency, and bodily ownership. A person may feel detached from the body, disconnected from ordinary identity, or separated from the surrounding world. These states show that selfhood is not a single fixed structure. It depends on integration among memory, body, emotion, agency, and perspective.
Such conditions are important because they reveal the fragility and complexity of self-consciousness. Consciousness is not merely sensory awareness. It includes the sense of being a subject, located in a body, embedded in time, and connected to memory and agency.
20.15 Comparative Evaluation Across Theories
Altered states are especially valuable because they test whether theories can explain both the presence and absence of consciousness, partial awareness, internally generated experience, and transformed selfhood.
Global Workspace Theory explains many altered states in terms of changes in global availability, reportability, and large-scale broadcasting [@baars1988; @dehaene2011; @dehaene2014]. It is strong in explaining why anesthesia or deep unconsciousness reduces reportable access.
Integrated Information Theory predicts that consciousness depends on integrated causal structure. It is especially relevant to anesthesia and disorders of consciousness, where measures related to complexity and integration have been used clinically [@tononi2004; @oizumi2014; @casali2013].
Recurrent Processing Theory emphasizes recurrent cortical feedback. It helps explain why sensory processing may continue unconsciously when recurrent stabilization is disrupted [@lamme2006].
Predictive Processing explains altered states through changes in hierarchical inference, prediction error, precision weighting, and self-modeling [@friston2010; @clark2013]. It is especially useful for dreams, hallucinations, psychedelics, and dissociation.
Higher-Order theories emphasize changes in metacognition, introspection, and awareness of mental states [@rosenthal2005; @lau2011]. They are relevant to lucid dreaming, meditation, and disorders affecting self-awareness.
Embodied and enactive theories emphasize bodily regulation, interoception, and organism-environment interaction. They are important for understanding anesthesia, dreaming, meditation, dissociation, and selfhood.
No single theory currently explains all altered states completely. Each highlights different dimensions of consciousness.
20.16 Ethical Implications
Altered and impaired states raise major ethical questions. Disorders of consciousness involve issues of personhood, suffering, autonomy, communication, medical decision-making, and end-of-life care. The possibility of covert consciousness makes these questions especially urgent.
If a patient is behaviourally unresponsive but retains awareness, then clinical care, communication efforts, pain management, and family decision-making may need to be reconsidered. Even uncertainty should encourage caution.
Anesthesia awareness also raises ethical concerns. Medical practice aims to prevent conscious experience during procedures requiring general anesthesia. Research into anesthesia and consciousness therefore has direct clinical importance.
Psychedelic and contemplative research also raises ethical questions, especially concerning vulnerability, informed consent, expectation, and interpretation of unusual experiences. Altered states can be scientifically valuable, but they must be studied responsibly.
20.17 Relation to the Hard Problem
Altered states help map the structure and mechanisms of consciousness, but they do not automatically solve the hard problem. They can show which brain states correlate with consciousness, how awareness disappears under anesthesia, how dreams are generated, or how psychedelics alter selfhood. But critics may still ask why any of these processes are accompanied by subjective experience [@chalmers1995; @chalmers1996].
For example, anesthesia research may explain how global access or integration breaks down. Dream research may explain how internally generated worlds are produced. Psychedelic research may explain how self-models become unstable. These are important explanations, but they may still leave open why such processes feel like anything.
Altered-state research therefore strengthens the empirical science of consciousness. It identifies dimensions, mechanisms, and dissociations. Whether it fully explains subjectivity remains a deeper philosophical question.
20.18 Strengths of Altered-State Research
Altered-state research has several major strengths. First, it is strongly empirical. It studies real changes in consciousness across clinical, experimental, and naturally occurring conditions.
Second, it has direct clinical relevance. Research on anesthesia and disorders of consciousness can improve diagnosis, care, communication, and ethical decision-making.
Third, it allows researchers to dissociate components of consciousness. Wakefulness, awareness, responsiveness, memory, selfhood, and sensory integration can be studied separately.
Fourth, it provides comparative tests for theories. A theory that explains only normal waking consciousness is incomplete.
Fifth, altered-state research connects neuroscience, philosophy, medicine, psychology, psychiatry, contemplative studies, and ethics.
20.19 Limitations and Challenges
Altered-state research also faces important challenges. One limitation is reliance on report. Many altered states involve impaired memory, communication, or behavioural responsiveness, making subjective experience difficult to assess.
A second challenge is measurement. Consciousness cannot be directly observed from the outside. Researchers must infer it from behaviour, neural activity, physiological markers, and later reports.
A third challenge is diagnostic uncertainty. Disorders of consciousness can be difficult to classify accurately, and misdiagnosis remains a serious concern.
A fourth challenge is subjective variability. Dreams, meditation, psychedelics, and dissociation can vary greatly across individuals and contexts.
A fifth challenge is ethical constraint. Researchers must be careful when studying vulnerable patients or powerful alterations of consciousness.
These challenges do not reduce the importance of altered-state research. They show why careful methods and humility are necessary.
20.20 Open Questions
Several questions remain unresolved. What neural mechanisms are necessary for consciousness under anesthesia? How can covert consciousness be detected reliably? What distinguishes dreaming from waking consciousness? How do psychedelic states alter self-modeling and perception? Can meditation reveal basic structures of awareness? How should disorders of consciousness be classified ethically and scientifically? Can altered-state research help solve the hard problem, or only map the mechanisms of conscious change?
These questions show why altered states remain central to consciousness studies. They are not side topics. They are essential tests of any theory of consciousness.
20.21 Evaluation
Anesthesia, disorders of consciousness, and altered states provide some of the strongest evidence that consciousness is multidimensional. They show that wakefulness, awareness, reportability, selfhood, sensory integration, memory, and responsiveness can dissociate.
Their greatest value is comparative. By studying how consciousness changes, weakens, disappears, and transforms, researchers can better understand its structure. Altered states reveal which features are necessary for ordinary consciousness and which can vary independently.
Their greatest challenge is interpretation. Because consciousness is subjective, researchers must infer its presence and structure indirectly. Behaviour, brain activity, and report all provide partial evidence, but none is perfect.
Altered-state research is therefore essential but incomplete. It deepens empirical understanding while leaving philosophical questions about subjectivity and the hard problem open.
20.22 Chapter Summary
Altered and impaired states of consciousness provide some of the most important empirical tests for theories of consciousness. They reveal that consciousness is not a single on-off state, but a multidimensional phenomenon involving wakefulness, awareness, reportability, memory, selfhood, sensory integration, and responsiveness.
Anesthesia shows how consciousness can be medically suppressed through disruption of neural communication, integration, and access. Disorders of consciousness show that wakefulness and awareness can dissociate. Covert consciousness demonstrates that some patients may retain awareness despite lack of behavioural communication.
Dreaming shows that consciousness can occur without ordinary external sensory engagement. Lucid dreaming shows that reflective awareness can vary within dream states. Psychedelic states alter perception, emotion, selfhood, and meaning. Meditation changes attention, self-awareness, bodily experience, and meta-awareness. Seizures and dissociation reveal the fragility of selfhood, memory, agency, and bodily ownership.
Different theories explain these states in different ways. Global Workspace Theory emphasizes broadcasting and access. Integrated Information Theory emphasizes causal integration. Recurrent Processing Theory emphasizes feedback loops. Predictive Processing emphasizes inference and precision weighting. Higher-Order theories emphasize metacognition. Embodied theories emphasize bodily regulation and lived experience.
The central lesson is that altered states are not peripheral to consciousness research. They are essential for testing theories, improving clinical care, and understanding the complex structure of conscious experience.